
COVID-19 Synthesis Phase 1 | 9 March 2020
COVID-19 Synthesis Phase 1 | 9 March 2020
Impossible Labs for doc.ai

Diagnostic Methods + Scaling Up Diagnostics
A variety of test options for COVID-19 are being developed, primarily a nasal swab/RT-PCR kit. Each test comes with its own set of benefits and drawbacks but the core issue in the US to date has been availability. We are seeing a lot of movement to make more test kits and other forms of diagnostics available to clinicians. However, the response is generally uncoordinated, which represents an opportunity to coordinate research, data and patients. In addition, we’ve identified two broad opportunities below and diagnostic-specific opportunities throughout.
Higher order opportunities:
Sync experts who are developing and deploying tests. What resources do they need? What can they learn from one another? What are they missing to have a faster rollout?
Possible to create a “detector” using multiple fast + cheap methods in conjunction?
Algorithm + multiple low-fi data sources for diagnosis (digital stethoscope, thermometer, heart rate, blood pressure, symptoms) . Lower radiation / partial CT scan, use a smaller dataset to fingerprint COVID19?
Diagnostic Methods
PCR
Many experts know how to develop and perform status quo RT-PCR swab COVID-19 testing. Independent efforts across the globe to make them open source. Additional nasal swab test kits are being made available. The Gates Foundation has also sponsored an at-home test kit. However, sensitivity is poor, resulting in a high rate of false positives/negatives. They also take 24-48 hours to turnaround results from centralized labs. Limitations of non-PCR testing require concentrated samples (156+ copies of virus) as minimum, whereas RT-PCR can work with only 1 copy.
Primer testing
Many sets of PCR primers used throughout the world, causing differences in accuracy and detection. WHO, CDC
ORF1 gene and N gene
Comparative analysis of primer-probe sets for the laboratory confirmation of SARS-CoV-2
Viral RNA extraction medium selling out, limiting access to researchers
Thermo Fisher paid $11B for Qiagen which has COVID19 test kit production: Thermo Fisher Is Buying Qiagen for $11.5 Billion. It’s a ‘Home Run’ Deal.
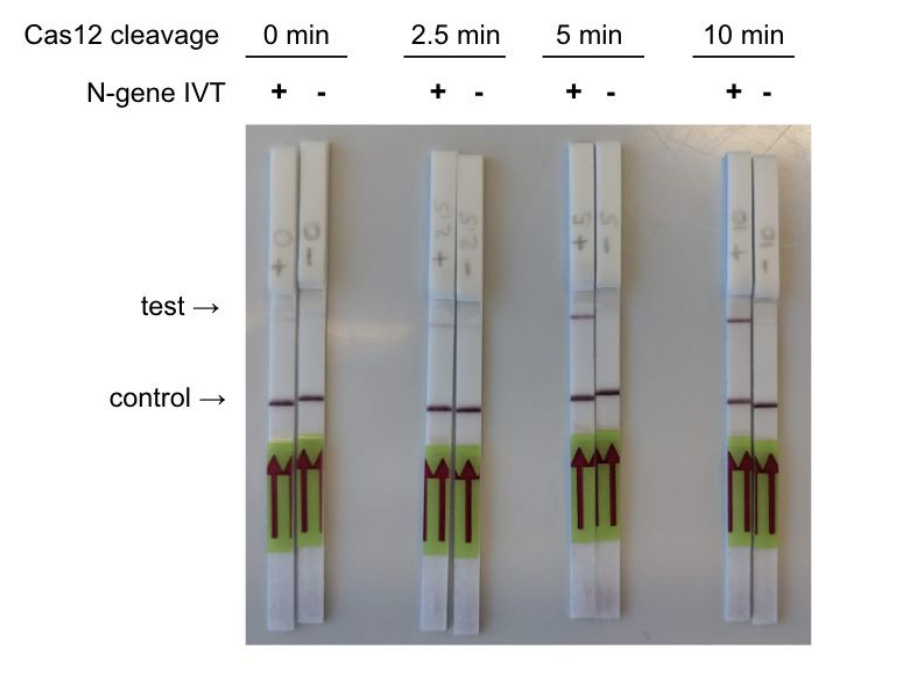
Isothermal amplification
CRISPR enabled 30 minute test vs 6 hours for RT-PCR
Requires 156+ copies present in sample. Does this mean it won’t work for early detection, more verification once someone is sick?
Jonathan Rothberg, working on isothermal PCR system. Sees convergence across DNA + Imaging + Pharma

Opportunity: Corral the PCR testing work being done by independent scientists into a single platform / tracking system
Opportunity: Patients who’ve tested positive share additional symptoms on doc.ai to get a fuller picture of health. Made available to researchers worldwide

Serological
Serological tests do better at identifying COVID-19 and require a blood sample. They look for specific antibodies that the body has produced to fight the virus. Singapore has developed an experimental antibody test for COVID-19 and China has licensed several. These are not yet available in the US. A serological test is advantageous because it can detect antibodies even if a patient has recovered, whereas a PCR test can detect the virus only if the person is currently sick. However, both tests might miss cases if samples are taken too early, when the viral load is too low or if the person's body hasn't produced antibodies against the virus yet
Opportunity: Capture population of sick AND recovering/recovered people. What can we learn from people who were affected but recovered? Vs people who did not recover?
Questions: Can we speed the availability of serological tests in the US? Can we send samples outside the US or do it ourselves without breaking laws?
Imaging
Imaging tests are generally performed at a later stage, specifically on the lungs, to detect ground-glass opacity
CT scan
2/26/20 Science Daily - CT provides best diagnosis for COVID-19
"About 81% of the patients with negative RT-PCR results but positive chest CT scans were re-classified as highly likely or probable cases with COVID-19, by the comprehensive analysis of clinical symptoms, typical CT manifestations and dynamic CT follow-ups,"
AI used to “screen patients and prioritize those most likely to have Covid-19 for further examination and testing”
Radiation risk from medical imaging, CT, chest: average effective dose = 7 mSv, range reported in literature 4.0-18 mSv
AI converts low-dose CT images to high-quality scans - 21 Jun 2019
A team of researchers from Rensselaer Polytechnic Institute (RPI) in Troy, NY, and Massachusetts General Hospital (MGH) in Boston developed a deep-learning model called a modularized adaptive processing neural network (MAP-NN), which progressively reduces noise on LDCT images with guidance from the radiologist until the optimal level of image quality is achieved. Testing on images from three different vendors, three radiologists found the algorithm produced images that were either better or comparable to images processed with iterative reconstruction. The deep-learning method also processed images much faster.
Google’s cancer-spotting AI outperforms radiologists in reading lung CT scans - May 22 2019
Qure, a startup focused on AI for medical imaging
qXR detects abnormal chest X-rays, then identifies and localizes 15 common abnormalities. It also screens for tuberculosis, and is used in public health screening programs.
Opportunity: doc.ai's team could create an AI diagnostic for COVID-19 using CT scan data. Could potentially do this faster by building an open source CT scanner. The risk is radiation exposure. Could machine learning be used to “fill in the gaps” in less robust images (aka less radiation used)?
Ultrasound
The findings on lung ultrasonography appear to correlate perfectly with the findings on chest CT scan. Sensitivity will depend on several factors (most notably disease severity, presence of obesity, and thoroughness of scanning).
“Low-cost” ultrasound is available starting at $2k. Butterfly iQ - Ultrasound, ultra-simplified.
Opportunity: Low-cost, open-source ultrasound with data shared among scientific community


MRI
“MRI scanning does not work well to take pictures of parts of the body that are moving, like your lungs, which move with each breath you take. For that reason, MRI is rarely used to look at the lungs.” (source)
Scaling Up Diagnostics
Human Clinical testing
Clinical labs
Tom Knight, co-founder of Ginkgo Bioworks,
Biologist army available for wet lab protocol testing, equipment
OpenMed Institute + OpenTrons robotic testing 2,400 samples per day:
OpenTRONS robot: How Opentrons Can Help Labs Screen Millions For COVID-19
Home testing
$1M incentive for home testing designs
Gates Foundation
400 tests per day capacity
Gates Foundation-backed program will soon be issuing home testing kits for COVID-19 in Seattle
Environmental testing
Sequence genomes to identify strain and mutations
Track prevalence of COVID19 strains worldwide
Thomas Landrain, Just One Giant Lab
Lots of volunteers coming in, but need PIs to direct it.
Looking for grant funding opportunities
Bill and Melinda Gates
Zuckerberg
Derek Jacoby
Environmental DIY testing
Treatment + Therapy
@HomodeusInc is working on getting a “home” - “pregnancy type” test for #covid19 to academic partners.
@aitherapeutics has sent a drug that inhibits coronavirus entry into cells to #Wuhan
Communication
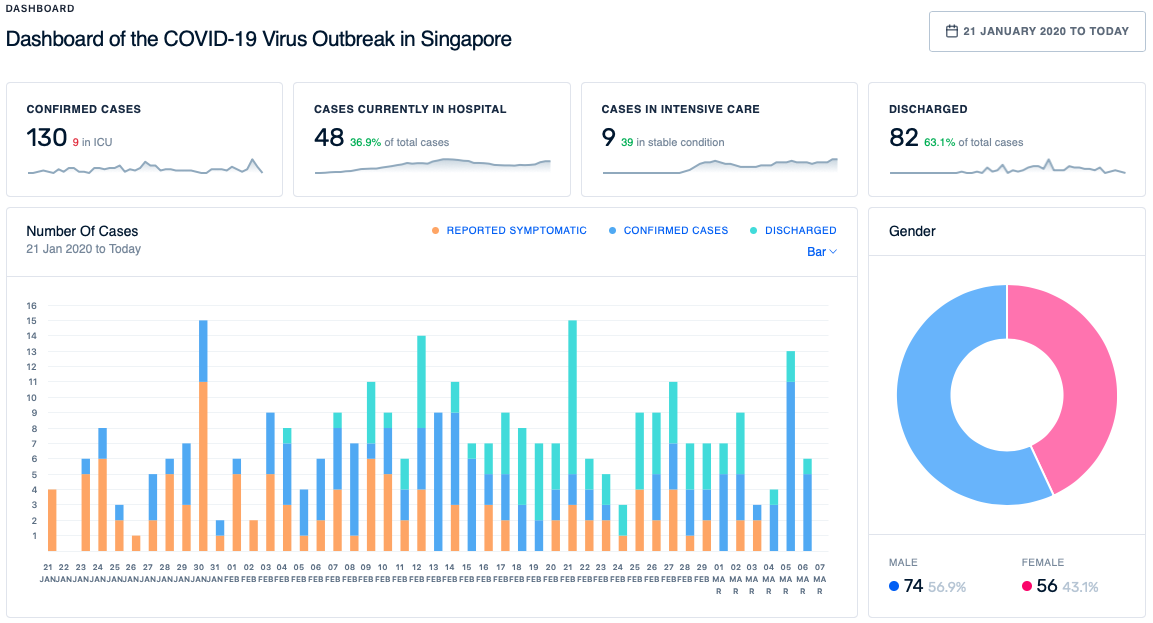
Dashboards
Dashboards connect disparate data and tell a story
https://www.technologyreview.com/s/615330/best-worst-coronavirus-dashboards/

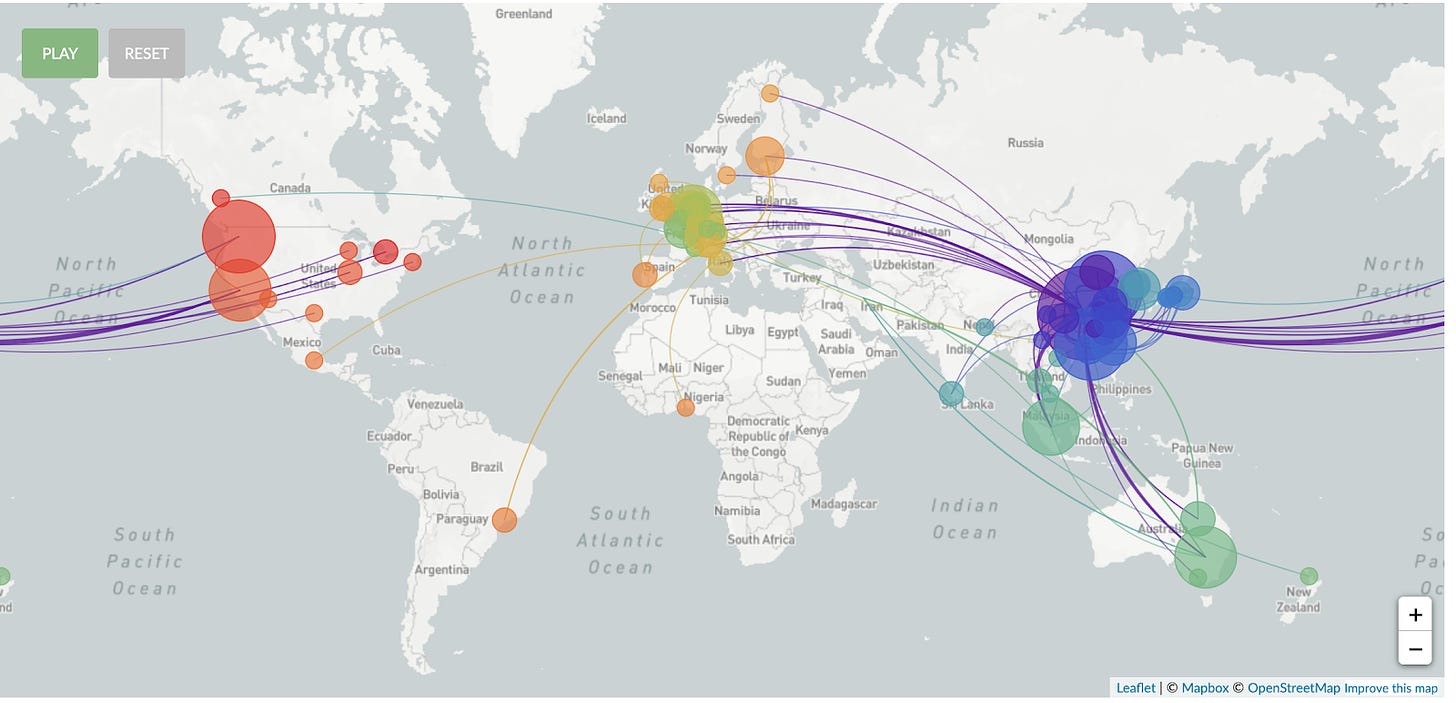
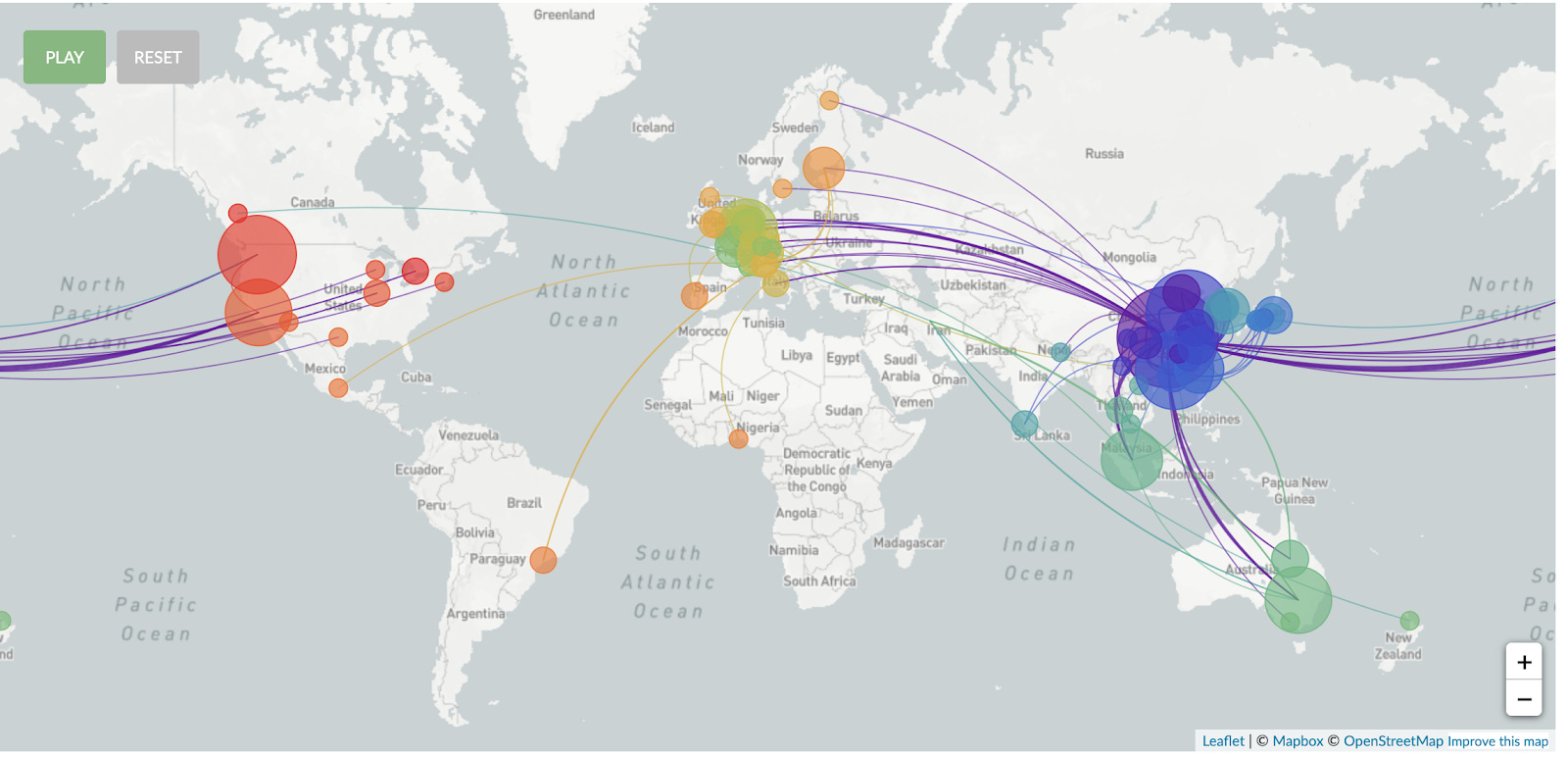
Animation of spread starting in December 2019: Genomic epidemiology of novel coronavirus (hCoV-19): https://nextstrain.org/ncov?l=radial
P.S. welcome to the doc.ai team. Comments welcome!
https://actionagainstcorona.org/
Is there not an association or collaboration between this effort and others, like the action against Corona Community ??